NEW DELHI, INDIA (IST)
00:00:00 PM
|
Loading...
DETECTING LOCATION...
00:00:00 PM
|
Loading...
| State | Life Expectancy (Years) |
|---|---|
| Hawaii | 80.7 |
| Washington | 79.2 |
| Minnesota | 79.1 |
| California | 78.6 |
| New York | 78.7 |
| Colorado | 78.5 |
| Idaho | 78.3 |
| Oregon | 78.1 |
| Utah | 78.0 |
| Virginia | 77.9 |
| North Dakota | 77.2 |
| Nebraska | 77.6 |
| Iowa | 77.5 |
| Wisconsin | 77.4 |
| South Dakota | 77.3 |
| Kansas | 77.1 |
| Michigan | 76.7 |
| Maine | 76.5 |
| Arizona | 76.4 |
| Montana | 76.2 |
| Wyoming | 76.1 |
| Nevada | 76.0 |
| Ohio | 75.8 |
| New Jersey | 75.7 |
| Georgia | 75.6 |
| Texas | 75.5 |
| Tennessee | 75.4 |
| South Carolina | 75.2 |
| Oklahoma | 75.1 |
| New Mexico | 74.5 |
| Pennsylvania | 74.4 |
| Florida | 74.6 |
| Louisiana | 74.0 |
| Alabama | 74.8 |
| Arkansas | 75.0 |
| Mississippi | 71.9 |
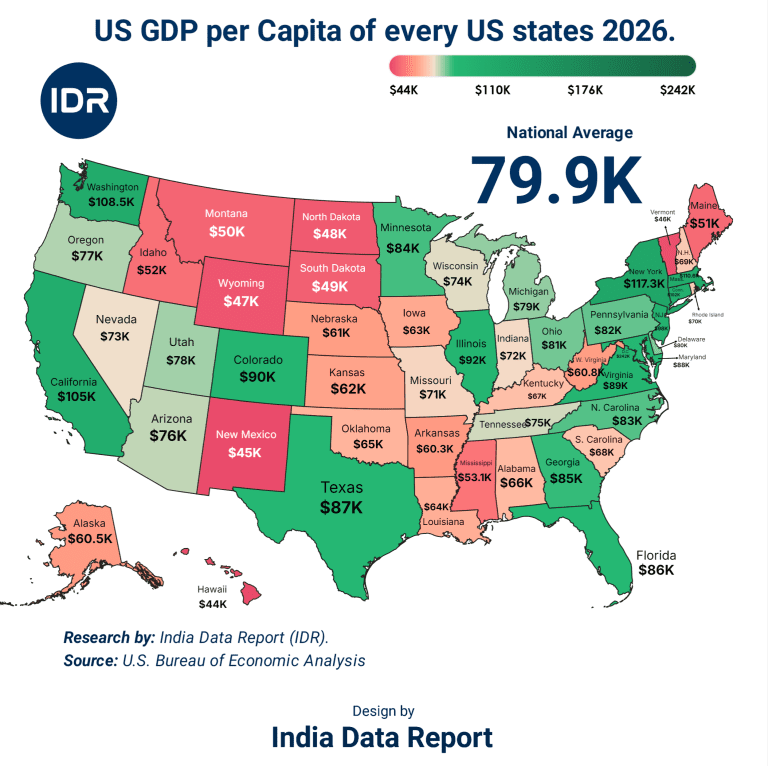
We are taught to believe that the ultimate measure of an economy’s success is its Gross Domestic Product, the soaring heights of its stock market indices, or the sheer volume of its industrial output. That is a lie. The only true currency of human civilization is time. Minutes, hours, years the baseline capacity of a human being to draw breath on this planet.
When you strip away the sanitized press releases from central banks and the triumphant speeches of politicians, you are left with a terrifying, raw reality: the global economic machine is actively trading human lifespan for capital efficiency.
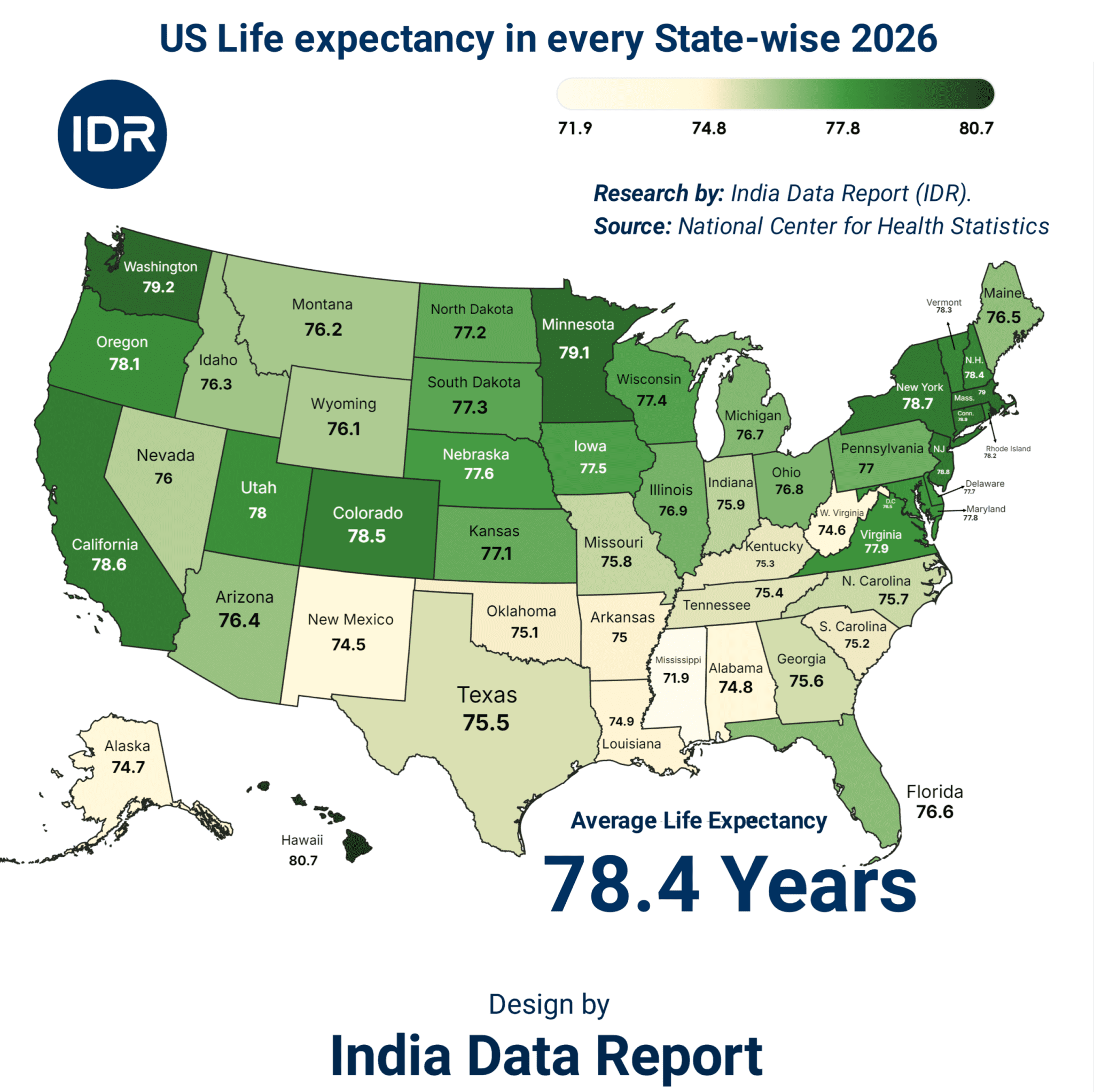
Look closely at the data released by the National Center for Health Statistics. On paper, it looks like a standard spreadsheet tracking life expectancy across different states. In reality, it is a ledger of economic warfare.
The national average stands at 78.4 years. But that average is a statistical ghost. It does not exist anywhere in reality. Instead, we see a chasm. A child born in Hawaii can expect to look out at the Pacific ocean for 80.7 years. Drive a few thousand miles into the American heartland, deep into the fractured industrial landscape of Mississippi, and that number collapses to 71.9 years.
That is nearly a nine-year penalty for being born on the wrong side of an economic boundary. Nine years wiped off the clock. In the world’s dominant superpower, survival is no longer a biological certainty; it is a premium tier commodity available only to those who can afford the subscription.
We live in an era of unprecedented technological marvels. We have artificial intelligence optimizing supply chains in milliseconds, mRNA platforms capable of rewriting immunotherapies on demand, and more billionaire wealth floating in private space programs than at any point in human history. Yet, a citizen in Mississippi has a shorter life expectancy than an individual living in many developing nations with a fraction of the per capita GDP.
How do we square this circle? The answer lies in the structural dismantling of the social contract. For the past four decades, economic policy has prioritized capital mobility over human resilience. When a factory closes in the Rust Belt or the Deep South, the financial markets cheer the “rationalization of assets.” What they fail to track is the immediate, measurable drop in local life expectancy that follows. Stress, nutritional poverty, substance abuse, and the outright collapse of rural healthcare infrastructure are the hidden line items on corporate balance sheets.
The data reveals a stark geographical caste system. The states flanking the coasts and the high-density tech hubs Washington (79.2), Minnesota (79.1), California (78.6), and New York (78.7) maintain a fragile hold on longevity. These are the regions where capital accumulates, where corporate healthcare packages shield professionals from the worst excesses of the system, and where tax bases remain robust enough to keep municipal water systems clean and public spaces viable.
Now look at the bottom of the ledger. The numbers do not lie, and they certainly do not care about political talking points.
| State / Region | Life Expectancy (Years) | Deviation from National Average (78.4 Years) | Economic Anchor / Threat Profile |
| Hawaii | 80.7 | +2.3 | High baseline tourism capital, isolated environment, robust public healthcare models. |
| Washington | 79.2 | +0.8 | Corporate tech cluster insulation, massive white-collar tax base. |
| Minnesota | 79.1 | +0.7 | Diversified agro-industrial base, historical investment in social safety nets. |
| California | 78.6 | +0.2 | Massive GDP generation alongside hyper-extreme wealth inequality. |
| Ohio | 75.8 | -2.6 | Industrial decay, legacy pollution, opioid epidemic epicenter. |
| Oklahoma | 75.1 | -3.3 | Resource extraction dependence, underfunded public medical infrastructure. |
| Louisiana | 74.0 | -4.4 | Environmental injustice corridor (“Cancer Alley”), chronic systemic disinvestment. |
| Mississippi | 71.9 | -6.5 | Absolute collapse of rural medical access, generational poverty traps. |
KADVA SACH (The Bitter Truth): A high national GDP means absolutely nothing when the bottom 20% of your population is dying at rates comparable to war zones. The top tier of states are effectively cannibalizing the resources of the interior, creating a dynamic where your wealth directly determines how many years you get to watch your grandchildren grow.
To understand why this chasm exists, we have to look past the charts and examine the human psyche. The current economic architecture operates on a fuel mixture of fear and greed. In hyper-competitive zones like New York or California, the fear of falling off the economic ladder drives individuals into 80-hour work weeks, chronic cortisol elevation, and sleep deprivation. They survive because they have access to elite concierge medicine, organic food deserts, and wellness structures designed to keep high-value corporate assets functioning just long enough to extract maximum productivity.
Conversely, in states like Mississippi, Alabama (74.8), and Louisiana (74.0), the fear is not about missing a promotion; it is the primal terror of a broken tooth turning into a lethal systemic infection because the local clinic closed down three years ago. When an economy treats healthcare as a profit center rather than infrastructure, preventive care vanishes. People do not go to the doctor when they feel a subtle ache; they wait until they collapse. By then, the cancer is stage four, the cardiovascular disease is irreversible, and the state’s life expectancy drops another fraction of a percentage point.
The old proverb says, “A healthy man wants a thousand things, a sick man wants only one.” Our current financial system, however, has realized that a sick man is an incredibly lucrative revenue stream. Chronic illness is far more profitable than either absolute health or sudden death. A patient managed through decades of expensive therapies, complex insurance bureaucracies, and high-interest medical debt represents a predictable, recurring cash flow for institutional investors. This is the dark secret of modern economic planning: there is a perverse financial disincentive to actually fix the underlying causes of regional mortality.
This systemic failure is hitting a critical inflection point as we move toward 2030. The automation of blue-collar labor, the consolidation of agricultural assets by corporate conglomerates, and the accelerating climate pressures on the Gulf Coast are converging. We are about to witness an exacerbation of this divide that no amount of cosmetic policy tweaks can fix.
When you map these metrics against regional economic policies, the correlation is undeniable. It is not a matter of climate or genetics; it is an direct reflection of state-level capital allocation decisions.
| Economic Zone | Avg. Lifespan Range | Primary Healthcare Delivery Model | Tax Base Stability | Vulnerability Index (Out to 2047) |
| Tier 1: Tech/Capital Hubs (HI, WA, MN, NY) | 78.7 – 80.7 Years | Highly consolidated, employer-subsidized, dense specialist networks. | Resilient, driven by global corporate earnings and real estate premiums. | Low immediate risk, high long-term vulnerability to structural hyper-inflation. |
| Tier 2: Agro/Resource Plains (ND, NE, IA, KS) | 77.1 – 77.6 Years | Decentralized, heavily reliant on critical access rural hospitals. | Moderate, tied tightly to global commodity price fluctuations. | Moderate risk of depopulation and medical professional flight by 2030. |
| Tier 3: Legacy Manufacturing (MI, OH, PA) | 74.4 – 76.7 Years | Fragmented, heavily burdened by legacy pension healthcare liabilities. | Declining urban cores with massive unfunded structural deficits. | High risk of accelerating mortality due to environmental toxicity. |
| Tier 4: Deep South / Extraction (LA, AL, MS) | 71.9 – 74.8 Years | Systematically underfunded, high rates of uninsured uninsured populations. | Weak, highly dependent on federal subsidies and regressive sales taxes. | Extreme systemic collapse risk; life expectancy projected to dip below 70 by 2035 without intervention. |
SUNHRA AVSAR (The Golden Opportunity): Corporations and visionary regional planners who pivot now toward decentralizing healthcare through autonomous regional clinics and localized organic food supply chains will capture a massive, untapped market. Saving these lives is not just a moral imperative; it is the single largest economic restructuring opportunity of the next quarter-century.
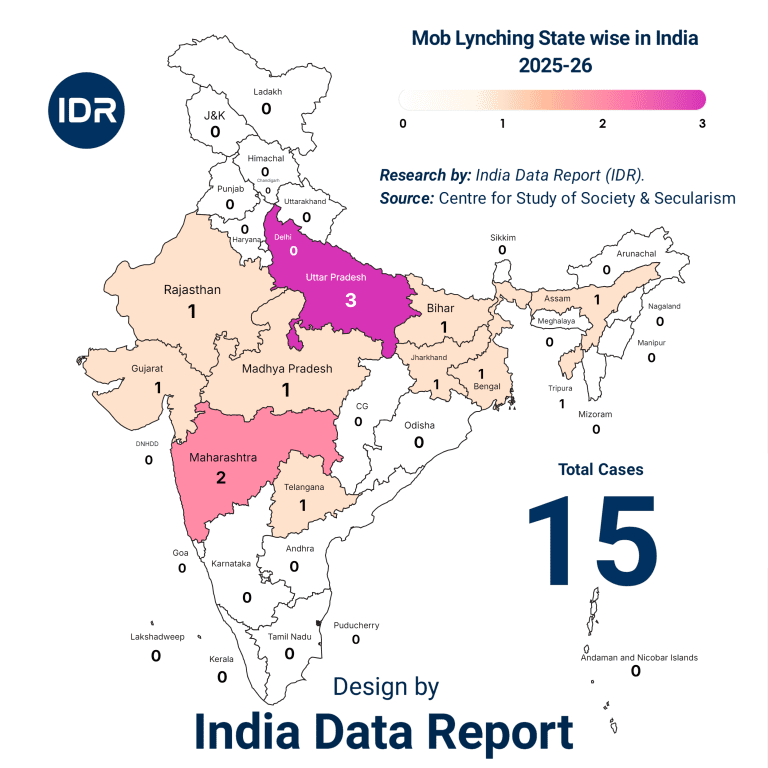
This structural rot is not isolated to western borders. The India Data Report (IDR) reveals an identical, chilling psychological mirror. As India pushes aggressively toward its 2047 vision of a fully developed economy (Viksit Bharat), the internal divergence is mimicking the American pattern with terrifying precision.
In high-income states and technology-driven urban centers like Kerala, Tamil Nadu, and parts of Maharashtra, life expectancy has climbed significantly, driven by rising literacy, private medical infrastructure, and stable middle-class wealth.
Yet, step into the deep rural interiors of the eastern belt regions heavily dependent on climate-vulnerable agriculture and raw resource extraction and the baseline numbers plummet. The hustle of Mumbai’s financial districts or Bengaluru’s tech corridors masks the stark reality of millions who are one major health crisis away from absolute financial ruin.
The global playbook remains unchanged: when a nation hyper-focuses on elite economic engines while letting its foundational healthcare infrastructure atrophy, it breeds a fractured populace. The lesson the IDR underlines is clear—whether it is Mississippi or a remote district in Bihar, the human body pays the ultimate price for unevenly distributed macroeconomic ambitions.
Let us stop pretending. The current trajectory is unsustainable. If left uncorrected, by the time we reach the centenary mark of 2047, we will not be looking at a single nation with regional differences. We will be looking at two distinct biological sub-species of human beings: an elite, long-lived coastal technocracy capable of pushing life expectancy past 85 through advanced bio-tech, and a short-lived, structurally neglected underclass in the interior whose lives are cut short before they hit 70.
This is not hyperbole; it is basic actuarial math. The current policy framework treats human life as an input expense to be minimized. To reverse this, we must fundamentally redefine what constitutes economic health.
By 2030: The life expectancy gap between Tier 1 and Tier 4 regions will widen from the current 8.8 years to an astonishing 11.5 years if federal Medicaid expansions remain blocked and rural hospital closures continue at their current run-rate.
By 2047: Longevity will become the primary driver of political unrest. Geodemographic secession where high-lifespan regions actively attempt to detach their tax bases from low-lifespan, high-liability regions will move from academic theory to mainstream political policy.
If you are an investor, a policy architect, or simply an individual trying to navigate this landscape, you must realize that the old paradigm of retirement planning is dead. You cannot save for a 30-year retirement if the very geography you inhabit is systematically shaving a decade off your life.
Capital Flight from Medical Deserts: Divest from real estate and long-term municipal bonds in regions showing consistent multi-year declines in baseline life expectancy. A community that cannot keep its healthcare infrastructure open is a community in terminal economic decline.
Decentralized Health Autonomy: Build personal and localized corporate resilience. Do not rely on institutional insurance structures that treat your longevity as a liability. Prioritize investments in preventative biometric tracking, sovereign water filtration, and regenerative agricultural access.
The New Balance Sheet: When evaluating career changes, corporate expansions, or family relocations, calculate the Geographic Longevity Premium. A job offering a 20% higher salary in an economic zone that shortens your life by five years is a net-negative transaction.
The clock is ticking. You can hide from the truth behind soaring stock market tickers and beautiful corporate quarterly reports, but you cannot negotiate with the actuarial tables. It is time to stop sacrificing our years on the altar of short-term capital efficiency. Demand systemic accountability, relocate your assets to zones that value human resilience, and treat your time as the only non-renewable resource it truly is. Turn this warning into your strategic playbook, or watch the economic machine claim your years next.